
Measles:
Vigilance after elimination
What not to miss this respiratory pathogen season
By Dr Varsha Sivalingam
Published June 2026
As we enter the winter respiratory season, clinicians appropriately focus on influenza, RSV and SARS-CoV-2. However, recent increases in global measles activity and intermittent local transmission in Australia highlight the importance of maintaining vigilance for this highly infectious disease. Early recognition and testing remain critical, not only for patient care but also for protection of the general public.
Although Australia achieved measles elimination in 2014, measles has not disappeared. Imported cases continue to occur every year, and during the past 12–18 months Australia has experienced an increase in both imported infections and secondary community transmission. During a busy winter season, when patients commonly present with fever, cough and coryza, measles can easily be overlooked unless clinicians actively consider it in the appropriate epidemiological context.
Why think of measles now?
Measles is caused by a paramyxovirus and remains one of the most contagious human infections, with a basic reproduction number (R₀) of 12–18. A single case in a susceptible population can rapidly lead to multiple secondary infections.
Table 1: Relative contagiousness of common infectious diseases (R₀).
| Disease | Approximate R₀ |
|---|---|
| Seasonal influenza | 1-2 |
| COVID-19 (original strain) | ~2-3 |
| Chickenpox | 8-10 |
| Measles | 12-18 |
The overlap between early measles symptoms and common winter respiratory illnesses creates a significant diagnostic challenge. The initial prodrome of fever, cough, coryza and conjunctivitis can be indistinguishable from influenza, RSV, adenovirus and other viral respiratory infections. This issue has become more important because the global epidemiology of measles has changed since the COVID-19 pandemic. Interruptions to routine childhood immunisation and catch-up vaccination programs during the pandemic led to a marked fall in global vaccine coverage. Large outbreaks have since occurred in Europe, Southeast Asia and parts of North America. Most Australian cases remain linked to overseas travel or contact with a returned traveller.
Measles vaccine was introduced in Australia in 1968, and widespread vaccination has dramatically reduced the incidence of disease. In 2014, the World Health Organization declared Australia free of endemic measles transmission. However, imported cases have continued to occur, and over the last year there have been several episodes of onward community transmission involving both vaccinated and unvaccinated individuals.
Figure 1: Annual notified measles cases by state and territory, Australia (past 10 years).
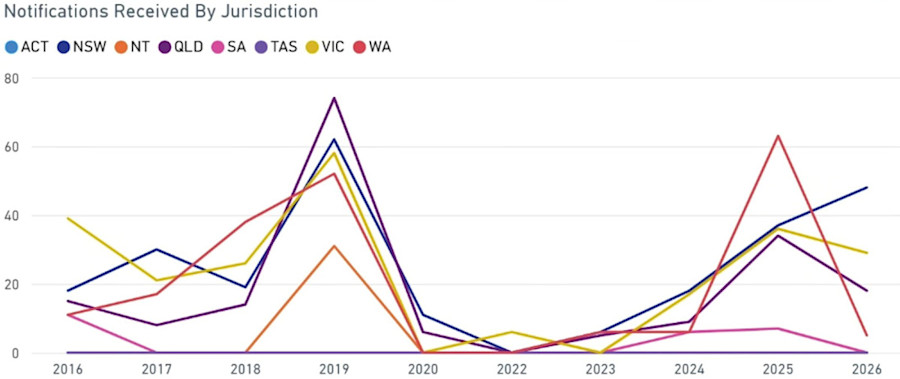
National Communicable Diseases Surveillance Dashboard, Assessed 10 June 2026.
What does measles look like?
Following exposure, measles typically develops after an incubation period of 10–14 days, although the range may be as short as 7 days or as long as 23 days. Illness begins with a prodromal phase lasting 2–4 days. During this period, patients usually develop a fever together with one or more of the classic “three Cs”: cough, coryza and conjunctivitis. There may also be atypical presentations with gastrointestinal symptoms.
Koplik spots are highly characteristic of measles and, when present, are considered pathognomonic. These are small bluish-white or white lesions on the buccal mucosa. They typically appear 1–2 days before the rash. However, they are not always seen, particularly if patients present late.

Image 1: Confluent maculopapular measles rash on the torso.
The characteristic measles rash is an erythematous maculopapular eruption that generally appears a few days after the onset of fever. The rash usually begins on the face before spreading downwards to involve the trunk, arms and legs. As the rash progresses, it may become confluent, particularly over the face and upper body.
Community transmission: why early detection matters
Measles is so contagious that even brief exposure can be sufficient for transmission. Recent Australian outbreaks have demonstrated that imported cases can rapidly lead to local transmission, particularly when diagnosis is delayed. Early recognition, immediate isolation and prompt notification to Public Health remain critical.
Although measles most commonly occurs in unvaccinated individuals, infection can occasionally occur in people who have previously received measles-containing vaccine, including those who have had two documented doses. These “breakthrough” cases may occur due to either primary or secondary vaccine failure. A single dose of a measles-containing vaccine is more than 95% effective, while two doses provide up to 99% protection against measles.
Primary vaccine failure is rare. Primary vaccine failure may occur due to failure to produce any humoral response to viral antigen (non-seroconversion) or problems with vaccine storage, cold-chain maintenance or administration. Patients with primary vaccine failure generally present with typical measles, including fever, cough, coryza, conjunctivitis and a classic rash.
Secondary vaccine failure occurs when a patient initially develops immunity after vaccination, but protection declines over time as antibody levels wane. Measles occurring in this setting is often termed “modified measles syndrome”. Some patients may present only with a febrile rash illness or mild respiratory symptoms. As a result, modified measles can easily be overlooked during influenza season. Patients with secondary vaccine failure generally have lower viral loads and are less infectious than unvaccinated patients with measles; however, transmission can still occur, and these cases remain important to identify.
Which patients should be tested?
Clinicians should maintain a low threshold for testing in patients with a compatible illness and relevant epidemiological risk factors. Testing should be strongy considered in patients with fever and a descending maculopapular rash, particularly when accompanied by cough, coryza or conjunctivitis, especially in the context of the following risk factors:
- Recent overseas travel, particularly to areas with known outbreaks or endemic transmission
- Contact with a suspected or confirmed measles case
- Infants too young to be vaccinated
Clinicians should also remember that measles does not always present classically. Increasingly, Australian cases are being recognised in partially immune individuals, who may present with mild or atypical symptoms.
An important point to note is that after receiving a measles-containing vaccine, people may develop a fever lasting two to three days, with associated malaise and a mild, non-infectious rash. The fever usually develops 7–10 days after vaccination (typically within 5–12 days). Approximately 15% of young children who receive the MMR vaccine experience a high fever (>39.4°C). Laboratory testing can distinguish wild-type (circulating infectious) measles from non-wild-type (vaccine strain) virus.
How to Order Measles Testing
Complete the Clinical Labs General Pathology Request Form, including the required tests below. For referrers in WA, please use the WA Request Form.
A combination of molecular and serological testing can be performed for suspected cases; however, polymerase chain reaction (PCR) testing is critical to confirm acute infection.
PCR is the diagnostic modality of choice early in illness and is most useful within the first few days after symptom onset, including during the prodromal phase before the rash develops.
Ideally, both a respiratory specimen and urine should be collected, as this increases diagnostic sensitivity.
Respiratory specimens required: 2 x nasopharyngeal swabs in viral transport medium (VTM)
1 swab specifically labelled for measles PCR (sent to the Public Health laboratory)
1 swab for routine respiratory multiplex PCR (sent to the local laboratory).* Visit our Respiratory Testing pages for state-specific ordering instructions.
Urine: Standard yellow-top container for measles PCR
It is important to notify the local Public Health unit of suspected cases so they can contact the lab to expedite testing.
*An important practical point is that routine respiratory viral PCR testing does not include measles. Given the overlap in symptoms between measles and other viral infections, it is good practice to also collect a sample for respiratory multiplex PCR.
Measles serology can be used to assess immunity and as an adjunctive diagnostic test in suspected acute infection. Suggestive features of an acute infection include identification of measles-specific IgM antibodies or demonstration of a rising titre of IgG antibodies in the absence of recent vaccination. In acute infection, serology (serum tube) should be collected at the time of illness, with convalescent serology performed two weeks later. A negative IgM result early in illness does not exclude measles. If clinical suspicion remains high, repeat serology and PCR testing.
Serum specimen required: Serum tube
Acute infection: IgM and IgG
Immunity assessment only: IgG
Respiratory Multiplex PCR Testing at Clinical Labs
Visit our Respiratory Testing pages for state-specific ordering instructions.
If you enjoyed this article, subscribe to our electronic Pathology Focus newsletter.
References
- Australian Centre for Disease Control. Measles, Australia and our strong vaccination record. Canberra: Australian Government Department of Health and Aged Care; 2025 [cited 24 April 2026]. Available from: https://www.cdc.gov.au/newsroom/news-and-articles/measles-australia-and-our-strong-vaccination-record
- Draper JL, Durrheim DN, Pillsbury AJ, et al. Measles epidemiology in Australia, 2014–2023. Commun Dis Intell (2018). 2024;48. Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/CA1DBF11D71F5F3ECA258ADE0019B036/$File/cdi-2024-48-62.pdf
- Moss WJ. Measles. N Engl J Med. 2025;393(2). doi:10.1056/NEJMra2504516.
- Rota PA, Bankamp B, Hickman CJ. Laboratory diagnosis and molecular epidemiology of measles in elimination settings. Emerg Infect Dis. 2024;30(9):1785-1794. Available from: https://wwwnc.cdc.gov/eid/article/30/9/24-0150_article
- Australian Centre for Disease Control. Measles. Canberra: Australian Government Department of Health and Aged Care; 2025 [cited 24 April 2026]. Available from: https://www.cdc.gov.au/diseases/measles
- National Centre for Immunisation Research and Surveillance (NCIRS). Measles vaccines frequently asked questions (FAQs) [Internet]. Sydney: NCIRS; [cited 24 April 2026]. Available from: https://ncirs.org.au/measles-immunisation/measles-vaccines-frequently-asked-questions-faqs
- Public Health Laboratory Network (PHLN). Measles: Laboratory case definition. Canberra: Australian Government Department of Health and Aged Care; 2009 [updated 7 December 2025; cited 24 April 2026]. Available from: https://www.cdc.gov.au/system/files/2025-09/measles-laboratory-case-definition_0.pdf
- Australian Technical Advisory Group on Immunisation (ATAGI). Measles. In: The Australian Immunisation Handbook [Internet]. Canberra: Australian Government Department of Health and Aged Care; 2026 [cited 24 April 2026]. Available from: https://immunisationhandbook.health.gov.au/contents/vaccine-preventable-diseases/measles
About the Author

Dr Varsha Sivalingam
FRACP FRCPA- Molecular Diagnostics
- Antimicrobial & Diagnostic Stewardship
- Integration of Genomics in Clinical Microbiology Practice
Dr Varsha Sivalingam studied medicine at the University of New South Wales and completed specialist training in Infectious Diseases and Clinical Microbiology at Nepean Hospital, Royal Prince Alfred Hospital and the Institute of Clinical Pathology and Medical Research (ICPMR), Westmead. She obtained Fellowships of the Royal College of Pathologists of Australasia (Microbiology) and the Royal Australasian College of Physicians (Infectious Diseases) in 2026.
Dr Sivalingam has a strong interest in molecular diagnostics, antimicrobial and diagnostic stewardship and the integration of genomics into clinical microbiology practice. She joined Australian Clinical Labs as a Clinical Microbiologist in 2026.
Local Pathologists
 Pathologist
Pathologist
 Pathologist
Pathologist
Related Pages

Navigating the National Cervical Screening Program
A clinical guide for GPs by Dr Catherine Uzzell and Kerryn Jones (FASC, CCS) covering HPV testing, risk‑based management and patient‑specific screening decisions.

Winter & Vitamin D Deficiency
Dr David Deam highlights how seasonal drops in vitamin D, particularly at the end of winter, underscore the importance of timely testing to support patient health and early detection of deficiency.

Thyroid Function Test Interpretation
Dr Phoebe Stanford explains how to interpret thyroid function tests accurately, addressing common pitfalls and interferences to improve diagnostic confidence.